In an illustration on page 2 chapter 1 , Palmer's point is shown, however; no explanation is given.
The following article is discussing the minimally invasive approaches through the abdominal wall in laparoscopy and you can find that in case of Central adhesion around the umbilicus, the Palmer's
point is considered to be the first alternative root to enter the laparoscopy port.
Article 1
Friday, August 17, 2007
URACHUS AND VITELLINE DUCT
The urachus is an embryological canal connecting the urinary bladder of the fetus with the allantois a structure that contributes to the formation of the umbilical cord. The lumen (inside) of the urachus is normally obliterated during embryonic development, transforming the urachus into a solid cord, a functionless remnant.

Allantois
This sac-like structure is primarily involved in respiration and excretion, and is webbed with blood vessles.
The function of the allantois is to collect liquid waste from the embryo, as well as to exchange gases used by the embryo.
In placental mammals, the allantois is part of and forms an axis for the development of the umbilical cord.
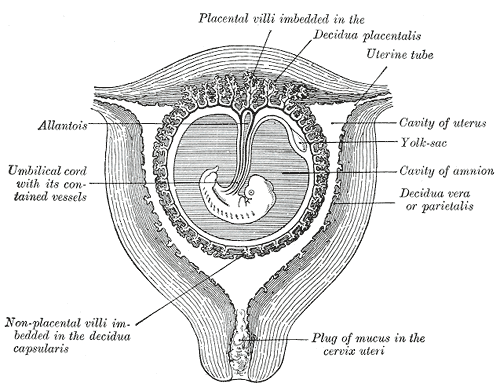
Vitelline duct
At the end of the fourth week the yolk-sac presents the appearance of a small pear-shaped vesicle (umbilical vesicle) opening into the digestive tube by a long narrow tube, the vitelline duct.
The vesicle can be seen in the after birth as a small, somewhat oval-shaped body whose diameter varies from 1 mm. to 5 mm, it is situated between the amnion and the chorion and may lie on or at a varying distance from the placenta.
As a rule, the duct undergoes complete obliteration during the seventh week, but in about three per cent of cases its proximal part persists as a diverticulum from the small intestine,
Meckel's diverticulum, which is situated about two feet above the ileocolic junction, and may be attached by a fibrous cord to the abdominal wall at the umbilicus.
Sometimes a narrowing of the lumen of the ileus is seen opposite the site of attachment of the duct.

UMBILICUS
The umbilicus is essentially a scar made from the remnants of the umbilical cord.
It is situated in the Linea Alba and in a variable position depending on the obesity of the patient.
however, the base of the umbilicus is the thinnest part of the abdominal wall and is the commonest site of insertion of the primary port in laparoscopy.
It is situated in the Linea Alba and in a variable position depending on the obesity of the patient.
however, the base of the umbilicus is the thinnest part of the abdominal wall and is the commonest site of insertion of the primary port in laparoscopy.
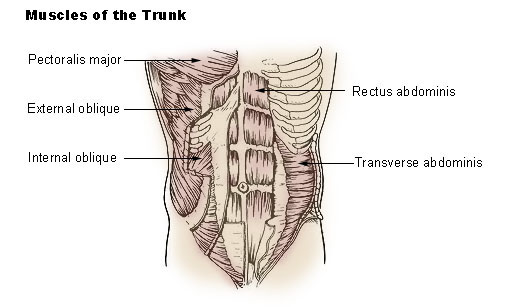
LINEA ALBA & PYRAMIDALIS MUSCLE
Where the abdominal muscles coalesce in the midline, linea alba is formed.
Pyramidalis muscle is present in all women origination on the anterior surface of the pubis and inserting into the linea alba.


Pyramidalis muscle is present in all women origination on the anterior surface of the pubis and inserting into the linea alba.


Monday, August 13, 2007

Wednesday, August 8, 2007
Chapter 1 : clinicl anatomy of the pelvis
The cutaneous nerve supply of the anterior abdominal wall arises from the anterior rami of the thoracic and lumbar vertebrae.
The dermatomes of the significant structures on the anterior abdominal wall are :
xiphisternum : T7
umblicus: T10
symphysis pubis : L1
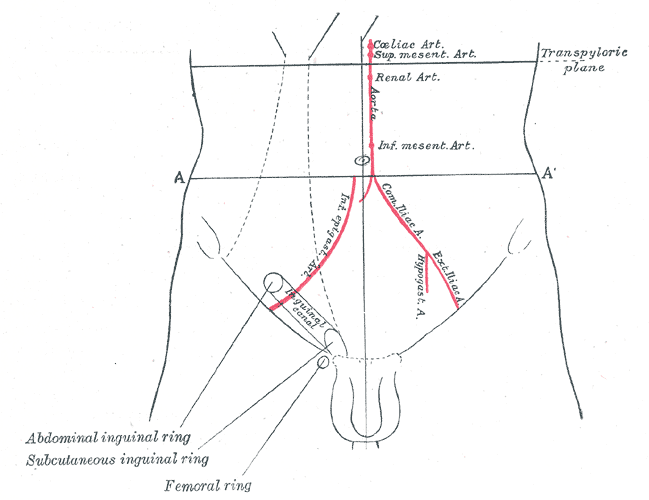
The blood supply is via the superior epigastric ( branch of internal thoracic artery ) and inferior epigastric artery ( branch of external illiac artery ) vessels.





The dermatomes of the significant structures on the anterior abdominal wall are :
xiphisternum : T7
umblicus: T10
symphysis pubis : L1
The blood supply is via the superior epigastric ( branch of internal thoracic artery ) and inferior epigastric artery ( branch of external illiac artery ) vessels.


Hello
Hi Sara
We are going to read the Dewhurst's textbook and we will make notes and discuss important points here in this weblog.
Bests of luck with your MRCOG exams
We are going to read the Dewhurst's textbook and we will make notes and discuss important points here in this weblog.
Bests of luck with your MRCOG exams
Subscribe to:
Comments (Atom)