Allantois
This sac-like structure is primarily involved in respiration and excretion, and is webbed with blood vessles.
The function of the allantois is to collect liquid waste from the embryo, as well as to exchange gases used by the embryo.
In placental mammals, the allantois is part of and forms an axis for the development of the umbilical cord.
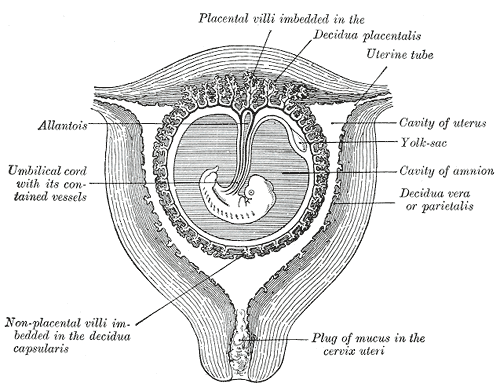
At the end of the fourth week the yolk-sac presents the appearance of a small pear-shaped vesicle (umbilical vesicle) opening into the digestive tube by a long narrow tube, the vitelline duct.
The vesicle can be seen in the after birth as a small, somewhat oval-shaped body whose diameter varies from 1 mm. to 5 mm, it is situated between the amnion and the chorion and may lie on or at a varying distance from the placenta.
As a rule, the duct undergoes complete obliteration during the seventh week, but in about three per cent of cases its proximal part persists as a diverticulum from the small intestine,
Meckel's diverticulum, which is situated about two feet above the ileocolic junction, and may be attached by a fibrous cord to the abdominal wall at the umbilicus.
Sometimes a narrowing of the lumen of the ileus is seen opposite the site of attachment of the duct.